The American Medical Association (AMA) published many changes impacting CPT® E/M codes and guidelines, which became effective Jan. 1, 2023. There are 25 deleted codes and many revisions to codes and guidelines in five code categories.
Overview
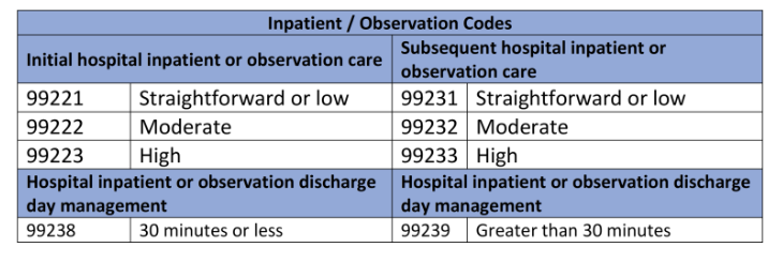
One of the most positive changes was the deletion of the observation E/M codes. CPT codes 99221-99223 and 99231-99239 will be used to report E/M services for both inpatient and observation status visits.
The guidelines for 2023 are essentially an expansion of the guidelines for 2021. When selecting the appropriate E/M level of service, medical decision making (MDM) or time will determine the overall complexity.
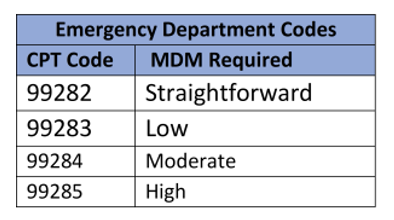
However, there is one exception to this rule that began January 1, 2023: All emergency department E/M codes will be leveled by MDM. Time-based billing is not permitted for emergency department codes (99281-99285).
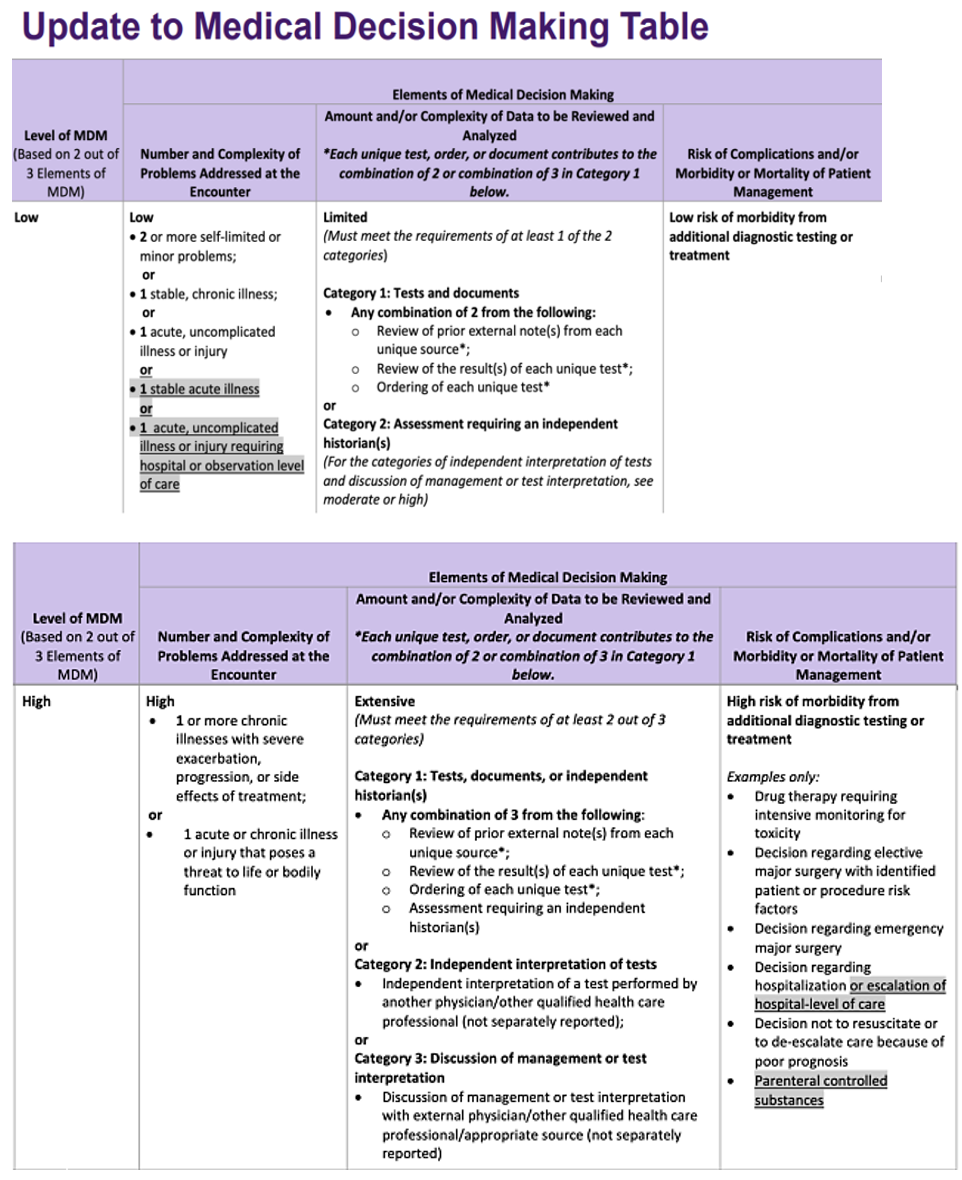
If you are familiar with the MDM table for the 2021 guidelines, you will find that the revised MDM table for 2023 is basically identical, with a few modifications to make it more suitable for inpatient E/M services.
In the column under “number and complexity of problems addressed,” CMS included a few more bullets, including one stable acute sickness and one acute uncomplicated illness or injury requiring hospital inpatient or observation level care.
- Stable acute illness is defined as “a new or recent problem for which treatment has been initiated.” The patient has improved and, while the condition has not been completely resolved, is stable.”
- Acute, uncomplicated illness or injury requiring hospital inpatient or observation level care is defined as “a recent or new short-term problem with low risk of morbidity that requires treatment.” There is little to no risk of mortality with treatment, and full recovery with no functional impairment is expected. In the “risk of complications and/or morbidity or mortality of patient management” column, they added parenteral controlled substances under the High MDM category.
Inpatient and observation care services
- Deletion of observation CPT codes (99217-99220, 99224-99226) and merged into the existing hospital care CPT codes (99221, 99222, 99223, 99221-99233, 99238-99239).
- Editorial revisions to the code descriptors to reflect the structure of total time on the date of the encounter or level of medical decision-making when selecting code level.
- Retention of revised Observation or Inpatient Care Services (Including Admission and Discharge Services) (99234-99236).
Based on the chart below, we can see that our moderate level observation example should be coded as 99222 in 2023. Furthermore, if the moderate level MDM patient is admitted to inpatient status the code should also be 99222.
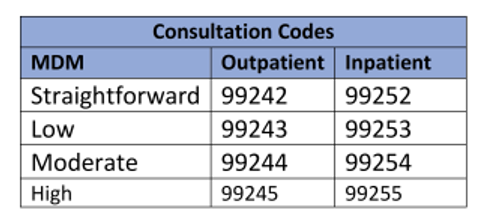
The consultation codes were also revamped. Just as they did with the 2021 changes, CMS removed the first level codes (99241 and 99251) to line up the four MDM levels (straightforward, low, moderate and high).
Consultations
- Retention of the consultation codes, with minor, editorial revision to the code descriptors.
- Deletion of confusing guidelines, including the definition of “transfer of care.”
- Deletion of lowest level office (99241) and inpatient (99251) consultation codes to align with four levels of MDM.
CPT Code 99281 for Emergency Department services were deleted and revised to an E/M code that does not require the presence of a physician or other qualified health care provider.
Emergency department services
- Maintained the existing principle that time cannot be used as a key criterion for code level selection.
- Editorial revisions to the code descriptors to reflect the code structure approved in the office visit revisions.
- Modified MDM levels to align with office visits and maintain unique MDM levels for each visit.
- Existing CPT code numbers maintained (analogous to office visit revisions).
- Articulated current practice that was not explicit in the CPT code set.
- May be used by physicians and QHPs other than just the ED staff.
- Critical care may be reported in addition to ED service for clinical change.
Nursing facility services
- Editorial revisions to the code descriptors to reflect the new standard E/M code structure.
- Revision to nursing facility guidelines with new “problem addressed” definition of “multiple morbidities requiring intensive management,” to be considered at the high level for initial nursing facility care.
- Deletion of code 99318 (annual nursing facility assessment). This existing service will be reported through the subsequent nursing facility care services (99307-99310) or Medicare G codes.
- Not all “initial care” codes are the mandated comprehensive “admission assessment” and may be used by consultants.
- Use subsequent visit when the principal physician’s team member performs care before the required comprehensive assessment.
Home and residence services
- Editorial revisions to the code descriptors to reflect the new standard E/M code structure.
- The domiciliary or rest home CPT codes (99334-99340) were deleted and merged with the existing home visit CPT codes (99341-99350).
- Elimination of duplicate MDM Level New Patient code (99343).
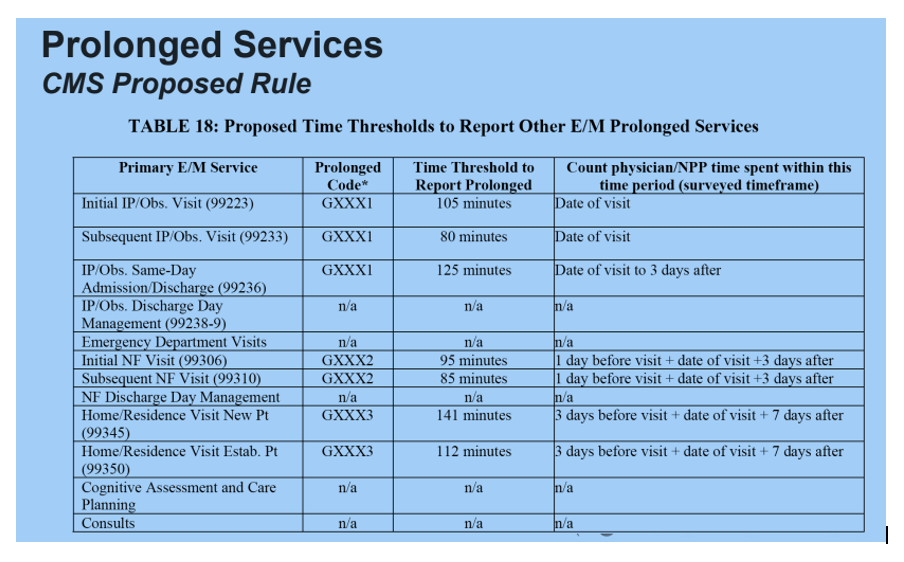
Prolonged services
- Deletion of direct patient contact prolonged service codes (99354-99357). These services are now reported through either the code created in 2021, office prolonged service code (99417), or the new inpatient, or observation or nursing facility service code (993X0).
- 99417 is also used for Home or Residence prolonged services.
- Creation of a new code (993X0) to be analogous to the office visit prolonged services code (99417). This new code should be used with the inpatient or observation or nursing facility services.
- Retention of 99358, 99359 for use on dates other than the date of any reported ‘total time on the date of the encounter” service.
 Conclusion
Conclusion
Keep these four points in mind to adapt to these changes:
- Medical decision making (MDM) tables are revised in which acuity or chronicity rather than quantity of disease/illness is addressed as complexity.
- Time-based coding is updated on many codes.
- Update the EHR to reflect deletions and revisions.
- Pay close attention to amended guidelines noted in the E/M section of the CPT® manual.
Click here for the AMA’s full overview of these changes.
Disclaimer: Accurate coding is the responsibility of the provider. This summary is intended only to serve as a resource to assist in the billing process.
Candice Chandler CPC, CEMC
Coding Services Manager
StreamlineMD